When patients ask whether they need an arm lift or just arm liposuction, they often frame it as a preference — a lighter option versus a more committed one. In reality, the decision is not preference-based. It is anatomy-based. The question that actually governs the outcome is not which procedure do I want, but what …


When patients ask whether they need an arm lift or just arm liposuction, they often frame it as a preference — a lighter option versus a more committed one. In reality, the decision is not preference-based. It is anatomy-based. The question that actually governs the outcome is not which procedure do I want, but what is limiting the silhouette of the arm.
The procedure should follow the diagnosis, not the other way around. In some patients, the arm looks heavy primarily because of fat thickness, and the skin still has reasonable recoil. In others, the dominant issue is skin laxity, and no amount of fat removal will tighten the envelope. Many arms sit somewhere in between, especially after weight changes or age-related loss of elasticity.
This article is not a pitch for one procedure over the other. It is an explanation of the clinical logic that determines which lever — if any — is honest for a given arm.
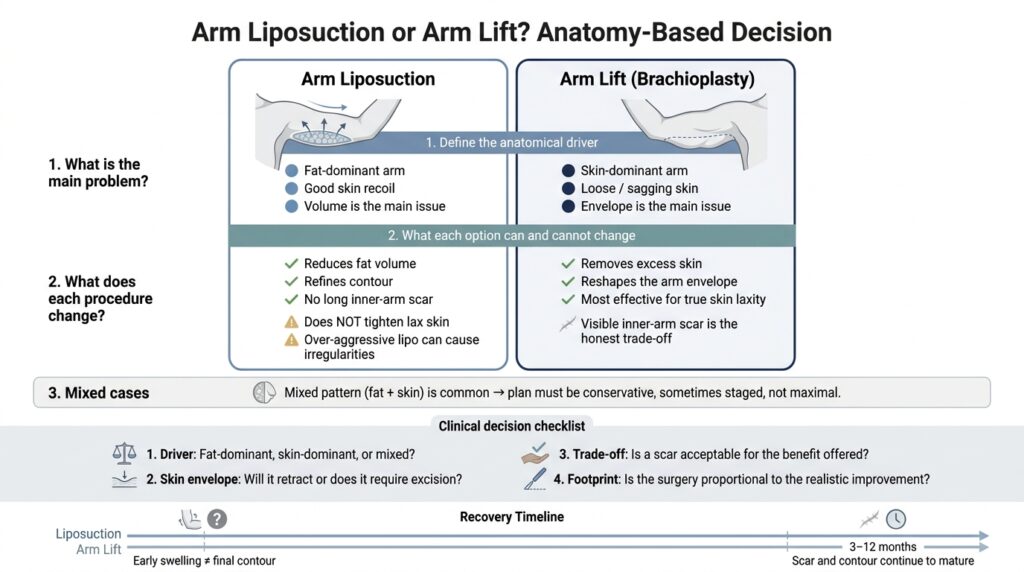
1) Define the problem before the procedure
Define the anatomical driver
The popular language of "lipo versus lift" collapses a nuanced anatomical question into a marketing choice. Clinically, the upper arm has three variables that matter: the fat compartment, the skin envelope, and the supporting fascia that tethers the skin to the underlying tissue. Each of these behaves differently, and only some of them respond to each intervention.
The fat compartment is what liposuction addresses. When fat is the dominant driver and the skin has good recoil, reducing volume can thin the arm and improve the line from shoulder to elbow. This is the scenario in which liposuction alone tends to deliver a clean result.
The skin envelope is a different problem. Skin that has lost recoil — whether through significant weight loss, repeated fluctuations, or age — does not retract reliably after fat is removed. In these arms, liposuction can actually make laxity more visible, because the internal volume that was holding the envelope outward is no longer there. The same loose skin is now draped over less support, and the arm can read as softer or more pendulous rather than tighter.
The dominant driver, then, is the governing variable. Naming it honestly — fat-dominant, skin-dominant, or mixed — is the diagnostic step that every procedural decision depends on.
2) Options (and trade-offs)
What each option changes (and what it cannot change)
Arm liposuction changes volume. It can thin a fat-dominant arm, refine the contour along the triceps, and improve the transition at the shoulder and elbow. What it cannot do is tighten a skin envelope that has already lost recoil. In patients with true skin laxity, expecting retraction from liposuction alone is not realistic, and overly aggressive fat removal in this setting tends to create irregularities rather than a smoother silhouette.
Arm lift (brachioplasty) changes the envelope. It removes redundant skin and, when indicated, a measured amount of fat along the excision plane. The honest trade-off is a scar along the inner arm. For skin-dominant arms, this scar is often the only mechanism that can meaningfully reshape the contour — because the problem is the envelope itself, and excision is the only reliable way to address it. For fat-dominant arms with good recoil, the scar is rarely a justified trade-off.
Mixed patterns are common, particularly after weight change or in arms with both thickness and laxity. In these cases, the plan has to be conservative. Aggressive combined contouring in a single stage can stress the skin, blur the border of the fat reduction, and produce exactly the irregularities the patient was hoping to avoid. A staged approach — or a smaller footprint in one stage — is often the more honest plan.
Before choosing a lever, it helps to convert the decision into a short set of clinical questions:
- Driver: What is the dominant anatomical driver — fat, skin, support, or a combination?
- Skin envelope: Does the skin have enough recoil to retract after volume reduction, or is excision the only honest lever?
- Trade-off: If a scar is required for a meaningful change, is that trade-off acceptable for the benefit on offer?
- Footprint: Is the proposed extent of surgery proportional to the improvement that is actually achievable?
If these questions do not have clear answers, the plan is not ready yet.
3) Recovery, timelines, and what "normal" looks like
Time-course realism
Arms are a visible, mobile area, and their recovery is not linear. Swelling after liposuction can persist for weeks and shift with activity and position; early thickness is not the final contour. After an arm lift, the scar passes through predictable but variable phases — firmness, pinkness, and gradual softening — that can take many months to settle. Early appearance is not final appearance.
Asymmetry in the early weeks is common and is usually a function of swelling rather than a structural problem. Patients who judge the result in the first month often underestimate how much change still unfolds between months three and twelve. In some patients, scars mature more slowly, and scar care is an ongoing part of the recovery rather than a one-time checklist.
Functional recovery — comfortable reaching, lifting, and sleeping — generally precedes aesthetic settling. This gap between feeling normal and looking final is part of the honest expectation.
The choice between an arm lift and arm liposuction is not a menu selection. It is the consequence of a specific diagnosis: fat-dominant, skin-dominant, or mixed, with a footprint that is justified by the benefit on offer. When the diagnosis is clear, the procedure tends to choose itself — and the role of the consultation is to make that diagnosis, not to default to the more familiar option.
A consultation exists to evaluate, not to commit. Waiting, optimizing weight, or deciding that no intervention is the right answer are all valid outcomes of an honest assessment.
Op. Dr. Mert Demirel
European Board Certified Plastic Surgeon (EBOPRAS)
ISAPS & ASPS Member
Istanbul, Turkey